There are about 50 million people on Medicaid in the United States and the biggest problem they have, by far, is finding a doctor who will see them. Yet this is actually an easy problem to solve if only the health policy community were not blinded by an overwhelming prejudice: The belief that for medical care to be accessible to low-income families it must be free at the point of delivery. In fact, the exact opposite is true. The quickest, surest way to create access to care for poverty-level families is to allow them to pay market prices.
A year or so ago I was in Boston and I struck up a conversation with a taxi driver, who informed me that she was on MassHealth (Massachusetts Medicaid). “How is it working for you?” I asked. “The biggest problem is finding a doctor,” she said. “I had to go down a list of 20 doctors’ names before I found one who would see me.”
“Were you going through the Yellow Pages?” I asked. “No,” she said, “I was going down a list that MassHealth gave me.”
Remember: this is what Massachusetts calls “universal coverage.”
Not only is access to care a big problem for Massachusetts Medicaid enrollees, it’s also a problem for people who are newly insured in subsidized plans sold in health insurance exchanges. According to a survey by the Massachusetts Medical Society:
- Only about half of internists (53%) and less than two-thirds of family physicians (62%) accept MassHealth.
- Only 43% of internists and 56% of family physicians will accept patients enrolled in Commonwealth Care (state-subsidized health plans).
- Only about one-third of internists (35%) and 44% of family physicians accept Commonwealth Choice (non-subsidized health plans).
- Only about half (50%) of pediatricians accept Commonwealth Care and only 45% accept Commonwealth Choice.
What is true in Massachusetts, is also true nationwide.
I previously reported on a finding that enrolling children in the Children’s Health Insurance Program (CHIP) does not result in their receiving more medical care. But when CHIP pays higher fees to doctors, the children do get more care. Suppose the state is strapped for money and can’t afford to pay higher fees? Common sense answer: let the parents add to the CHIP reimbursement rate and pay a higher price. The obstacle to common sense: it’s illegal for parents to do this. In fact, it’s more than illegal. It’s actually criminal. [I know the doctor receiving the money could go to prison. Could the parents paying the money go to prison as well? If you know, tell us in the comments section.]
Think about that for a moment. We encourage families to enroll their children in CHIP, by making the coverage free. Many apparently drop their private coverage to take advantage of the opportunity.Then, when access to doctors declines and the time doctors spend with these patients declines as well, we make sure they have no other options. We make it illegal for the family to pay the market rate for their care!
When we expand a government insurance plan for low-income patients, we are spending billions of dollars in a way that doesn’t increase access to care. At the same time, we forbid the enrollees to do the one thing that would expand access to care.
Contrast this foolishness with the Food Stamp program (SNAP), which also has about 50 million participants. Low-income shoppers can enter any supermarket in America and buy almost anything the facility has to offer by adding cash to the “voucher” the government gives them. They can buy anything you and I can buy because they pay the same price you and I pay. But we absolutely forbid them to do the same thing in the medical marketplace.
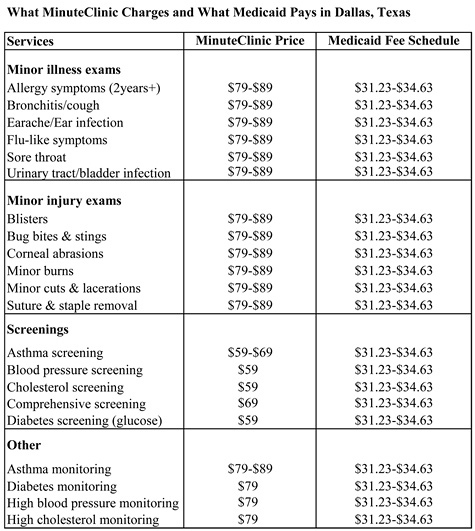
Take a look at the table below. It compares the prices charged by MinuteClinic to the rates Medicaid pays in Dallas. In general, Medicaid pays less than half. That’s why MinuteClinics usually don’t accept Medicaid. If low-income families were allowed to add from $30 to $50 of their own money to the Medicaid rate, however, in one fell swoop we could make high-quality, very accessible primary care available to millions of people.